New Discoveries in Cancer and Heart Disease

DISCOVERING MCED
The discovery of MCED involves insight, serendipity, and a bit of drama
Dr. Weisenthal says the discovery process began while he was performing a laboratory test he invented - the Weisenthal DiSC Assay - on behalf of a cancer patient whose illness was not responding to treatment. Dr. Weisenthal’s laboratory is largely focused on finding effective treatments for individual cancer patients, especially those in difficult situations.
Peering though a microscope for several hours, Dr. Weisenthal was examining this patient's cancer cells. The cells were mounted on glass slides and stained with dyes to highlight cellular structures. The cells had been removed from the patient's body by means of a biopsy procedure. Dr. Weisenthal’s purpose in viewing the cells was to observe the effect of a wide range of chemotherapy drugs to which the cells had been exposed. The cancer cells were still living at the time of exposure to the drugs. By determining which drugs were effective at killing this patient's cancer cells and which drugs were not effective, Dr. Weisenthal could then tell the treating physician which chemotherapy regimens afforded the best chance for patient benefit and which regimens should be avoided.
Each slide he reviewed for this patient displayed the same cellular features Dr. Weisenthal had encountered hundreds of thousands of times over a 40 year career as a medical oncologist and cancer researcher. But then something caught his eye. It was pattern of staining; broad smudges of violet not generally associated with slides prepared and stained in this manner.
After eliminating the possibility of cellular debris or some sort of staining artifact Dr. Weisenthal realized he was looking at endothelial cells. Endothelial cells form the linings of blood vessels: arteries, veins, capillaries, and heart valves. More precisely, as Dr. Weisenthal subsequently concluded, the smudges were patterns of calcium staining. Moreover, these patterns were associated only with endothelial cells that died in a very distinctive way. And what makes the story interesting is that the way in which these particular endothelial cells had died was a type of endothelial cell death unknown to science before Dr. Weisenthal discovered it that night.
Tissue Microaggregates and Personalized Medicine
In order to understand how smudges calcium staining in proximity to cancer cells relate to a discovery in heart disease it is necessary to understand the nature of the biopsy specimen Dr. Weisenthal had been examining.
Dr. Weisenthal's lab performs personalized cancer cytometric testing. Here's how it works:
In the case of what is called a “solid” tumor type, such as breast, lung cancer, colon, pancreatic, or ovarian cancer, a tumor mass, containing living cancer cells, is surgically removed from the cancer patient. The biopsy specimen is placed immediately into sterile medium - a liquid mixture of life-sustaining ingredients. The specimen is then conveyed to Dr. Weisenthal’s laboratory by overnight courier. Upon arrival at the lab, a variety of techniques are applied to reduce the specimen to an almost pure concentration of living cancer cells. Note the distinction "almost pure" becuse it is very important.
The cancer cells are not completely isolated. Instead, they are maintained as tiny, three-dimensional clusters, called microaggregates, in order to preserve important cell to cell signaling. The microaggregates containing the still-living cancer cells are then distributed among the wells - shallow indentations about half the diameter of a pencil eraser - in a rectangular, plastic (polypropylene) microtiter plate.
There are 96 individual wells on each plate. A different chemotherapy drug, or combination of drugs is added to the microaggregates in each well.
The plates, containing cells and drugs, are then placed in a temperature and CO2-controlled incubator for 96 hours. At the end of the drug exposure period, the cells are deposited on glass microscope slides through a process called cytocentrifugation. Biological stains are then applied. These are special chemical dyes that color-stain various cellular features, making them easier to see.
At this point Dr. Weisenthal examines the stained cells under a microscope to assess the effect of each chemotherapy drug upon the cancer cells. This enables the cancer patient to receive a chemotherapy treatment, personalized for him or her, that offers the best chance for remission or cure.
Now let’s return to the discovery. As it turns out, in addition to cancer cells, Dr. Weisenthal’s microaggregates also contain endothelial cells. Dr. Weisenthal was able to confirm the identity of these cells using special biochemical stains that react preferentially to this type of cell. The obvious question is, why did he notice the endothelial cells on the night of dicovery when he had not noticed them in all the years before? It was because of an extraordinarily vivid pattern of staining displayed by the endothelial cells on that one, specific microscope slide. Okay, so why did these particular endothelial cells stain so unusually vividly? For that matter, why had other researchers not discovered this particular staining pattern previously? There are three reasons that explain these questions - and here’s where serendipity comes into the picture.
Serendipity
First, let’s address the question of why earlier researchers had not discovered the vivid staining pattern that pointed to a previoulsy unknown manner of endothelial cell death.
There is a term called “cell culturing” that refers to the process of keeping cells alive in the laboratory after they are removed from a living host. Cell culturing generally involves the use of what is called a medium. Typically, this is a liquid substance containing ingredients that help to sustain living cells.
People whose job it is to study endothelial cells use a special type of culture medium that was painstakingly designed to stop endothelial cells from dying while they are undergoing study in the laboratory. As Dr. Weisenthal’s later experiments were to reveal, this endothelial cell culture medium is especially good at inhibiting MCED. MCED is an abbreviation that stands for Massively Calcified Endosome Death. It is the name Dr. Weisenthal assigned to the previously-unknown type of endothelial cell death that is the object of his discovery. And so, since the culture medium used by other investigators specifcally inhibited MCED, is it entirely understandable that no other investigators were able to observe MCED.
Recall, however, that Dr. Weisenthal was not intending to study - or culture - endothelial cells. As a matter of fact, he didn’t realize endothelial cells were even present in his cancer cell microaggregates. They just happened to be there - “hitch-hikers,” as he now calls them. The type of cell culture medium used by Dr. Weisenthal was designed to sustain cancer cells, not endothelial cells. Since there was nothing in Dr. Weisenthal’s culture medium to prevent the occurrence of MCED (which only affects endothelial cells and not cancer cells), many of the hitch-hiking endothelial cells on this one particular slide - more about that in a moment - underwent MCED-mediated endothelial cell death. This, in turn, is what caused them to display the vivd staining pattern that caught Dr. Weisenthal’s eye.
Two Types of Cell Death
We probably should say a word here about that vivid staining pattern and what caused it. A defining feature of MCED, as opposed to to the previously known type of endothelial cell death, is the gradual accumulation of large amounts of calcium. In non-MCED cell death, calcium levels spike and then dissipate rapidly in a matter of seconds or minutes. In MCED-mediated cell death, calcium levels rise steadily over several hours. This meshes nicely with Dr. Weisenthal’s 96 hour drug-exposure method. It is another serendipitous aspect of the MCED discovery. It is precisely this large volume of accumulated calcium that stained so vividly on Dr. Weisenthal’s cancer slide.
Why Didn’t Dr. Weisenthal Discover This Sooner?
Now for the other question. In 35 years of studying cancer cell microaggregates why did Dr. Weisenthal not notice the MCED staining pattern prevoisly? The answer to that must be told in two parts - and here is where the improbable truly occurs.
The first part of the answer may seem a bit dry. It will seem less so, however, when combined with the second part. It also figures largely in a maddening puzzle that presented itself later and nearly sank the entire discovery. But first things first.
We mentioned earlier that endothelial cell culture medium contains, almost by accident, MCED inhibitors. We say “by accident” because the developers of the medium did not know about the existence of MCED - they knew only that their medium was good at keeping endothelial cells alive. Also by accident, although Dr. Weisenthal did not know it at the time, some - but not all - batches of a specific ingredient Dr. Weisenthal had been using for many years in his lab’s home-brewed cancer cell culture medium also contained these same anti-MCED factors. It was entirely luck of the draw, as later experiments were to confirm, that the particular cells upon which Dr. Weisenthal made his discovery had been cultured in a batch of medium that did not contain the occult anti-MCED factors.
That was the technical part. Here is where things become a little more interesting. In retrospect, Dr. Weisenthal now refers to the cancer specimen upon which the MCED discovery was made as “MCED Specimen Zero.” It is the starting point for a series of follow-on discoveries involving other human tissue specimens.
Pancakes
MCED Specimen Zero happened to come from a neuroendocrine tumor, a relatively rare cancer involving hormone-producing cells. The specific tumor type isn’t important. What is important is that these cancer cells, when tested in the laboratory, were tenaciously resistant to injury by any of the chemotherapy drugs tested against them - bad news indeed for this particular patient. As Dr. Weisenthal labored his way through the patient's glass microscope slides - more than 50 of them - he saw that slide after slide was crowded with undamaged cancer cells. Stained pink and viewed through the micoscope, the cells were big and fully-intact. It was like performing a close-up inspection of a Monet painting in which all of the lily pads were colored bright pink. Actually, Dr. Weisenthal uses a different metaphor. He describes the unaffected cancer cells as big pink pancakes. And, because these cells had all been exposed to standard chemotherapy drugs, designed to kill cancer cells and not endothelial cells, any endothelial cell death occuring on these slides would have been extremely rare, largely obscured by the abundance of intact cancer cells, and, if noticed at all, easily mistaken for cellular debris.
Chance Occurrence
But the last slides Dr. Weisenthal examined for this patient were different. The cells on these slides had been exposed to a drug called bevacizumab. Bevacizumab’s main purpose is not to kill cancer cells directly. Bevacizumab works by depleting a substance called vascular endothelial growth factor, commonly abbreviated as VEGF. Without VEGF, endothelial cells die. Why should an anti-cancer drug target endothelial cells? We will explain it just a little farther along. Meanwhile, our story has finally reached its climax - the precise moment of discovery.
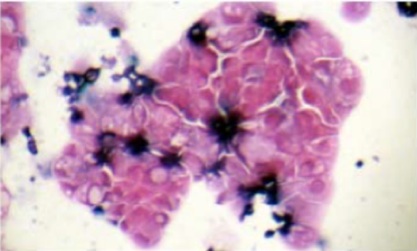
When Dr. Weisenthal viewed this slide he found it crowded with pink tumor cells as before but he also found, scattered among the tumor cells, an abundance of deep purple splotches. Here is how Dr. Weisenthal describes it, using his “pancake” metaphor:
“So, basically, I looked at close to 50 cytospins in a row and they were all monotonously the same - filled with nice clean, pink pancakes. The very last slides were the bevacizumab slides. They looked different. Instead of being filled with plain pink pancakes, they were filled with pink blueberry pancakes.”
Opportunity
At first, Dr. Weisenthal was puzzled as to the meaning of this unusual staining pattern. He circled back and reviewed hundreds of archival slides among the tens of thousands in his library. These had been created by Dr. Weisenthal in the past while performing chemotherapy drug testing for legions of former cancer patients.
Dr. Weisenthal then set about conducting hundreds of individual experiments, very often using his own blood. A visitor to the lab in those days would have been hard-pressed to find Dr. Weisenthal without a cotton ball taped over an artery on his forearm. The same fate often befell one or more members of his lab staff. The experiments involved using different staining methods, different cell culture techniques, different types of chemotherapy drugs, sera from different human donors, and exposing the cells to many different chemical agents to see what would happen. He scoured the medical literature, looking for clues that might help to corroborate or refute theories that were beginning to crystalize in his mind.
Finally, as the picture became increasingly clear, Dr. Weisenthal recognized that he had discovered a brand new mechanism of endothelial cell death - one that had never been described in the medical literature. He named the new mechanism MCED - Massively Calcified Endosomal Death. And so now he had a new mechanism and also a new name for it. But what did it all mean?
MCED in Cancer Treatment
As a cancer physician and researcher, it first occurred to Dr. Weisenthal that he had just invented an excellent test to guide the use of a new class of anti-cancer agents called angiogenesis inhibitors. Bevacizumab, discussed above as the drug that produced the “blueberry pancake” slide, is one of these drugs. Anti-angiogenic drugs work by interfering with the growth of capillaries that deliver oxygen and nutrients to the cells in a tumor mass. The capillaries also allow for removal of waste products and serve as routes by which cancer cells metastasize to other parts of the body. In theory, destroying the capillaries starves tumor cells of life-giving blood and the cells die.
The problem with these promising new anti-angiogenic drugs is that they don't work for everyone and when they do work they typically do so for only a while and then they stop working altogether. Also, anti-angiogenesis drugs are enormously expensive and they often produce dangerous side-effects. And so a way was needed to determine exactly which patients would benefit from anti-angiogenesis drugs and which patients would not benefit from them. Dr. Weisenthal’s new test seemed to afford an ideal solution.
Another Critical Discovery
And so Dr. Weisenthal’s MCED research moved forward. Further exhaustive experimentation and a lot of innovative deduction led Dr. Weisenthal to the conclusion that specific factors - substances that could be detected in the blood - are associated with the occurrence of MCED. Importantly, he also discovered that different human sera - essentially, blood from different individuals - have differing abilities either to promote or inhibit MCED. But still, what does that have to do with heart disease?
MCED in Heart Disease
Despite much progress made in the prevention and treatment of heart disease, it remains the leading cause of death worldwide. Moreover, many mysteries remain unsolved. Why, for example, do some persons with high serum lipid profiles - high amounts of cholesterol and other fatty acids in their blood - have lovely, unobstructed arteries while other persons, whose serum profiles are deemed favorable, suffer arterial blockage, heart attack, and stroke? High cholesterol is often associated with heart disease but, inconveniently, not always. Why is that? Clearly, cholesterol seems to be a factor but just as clearly it is not the main factor.
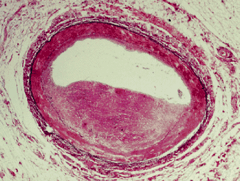
It is also not completely understood by scientists exactly what causes vessels to become inflamed. Inflammation, by the way, is a more accurate way of referring to the narrowing of an artery. It is now fairly universally understood that fat does not literally become deposited on the inner walls of blood vessels like sludge in an old sewer pipe. Instead, the wall of the vessel itself undergoes an apparent thickening as part of an inflammatory process. This causes the lumen, the channel in the middle of the vessel through which blood flows, to become progressively narrower until, one day, a turbulent fluttering of blood against the narrowed, uneven surface of the vessel wall serves as a signal to summon platelets. In keeping with their assigned function, the platelets dutifully form a blood clot. In most cases this platelet recruiment clotting system is highly-useful. It is the same mechanism that stops a minor cut from bleeding endlessly. However, when it happens inside an artery, it delivers a potentailly fatal blow in the form of a heart attack or stroke, depending upon where the clot occurs or ultimately lodges.
The New Mechanism
What causes this inflammation to occur? A few theories have been proposed and these have achieved varying degrees of acceptance within the scientific community. However, all of the theories fall short in accounting for apparent contradictions which are known to exist in the genesis and behavior of atherosclerosis. All of the theories fall short, that is, except one.
MCED appears to explain everything. In fact, having formulated his MCED hypothesis, Dr. Weisenthal then undertook a series of experiments ruthlessly designed to disprove it. Far from refuting the hypothesis, each experiment revealed yet another insight that seemed to support it. The most recent of these insights - enhancements to the original hypothesis which more fully elucidate the MCED mechanism - only recently emerged. (Click on the slide at right to see a larger view. For a 4 minute video, click here.)
Before moving on, it might be useful to recap where things stood just before the new insights came to light.
MCED Discoveries, 2006 - 2013
Without becoming overly-technical, here is where things stood with respect to Dr. Weisenthal’s conclusions as of late 2013. If you wish to read more detail, kindly consult the PUBLICATIONS page of this website. Links to Dr. Weisenthal’s MCED journal articles, abstracts, and poster presentations are provided. The earlier publications will not reflect insight acquired and published by Dr. Weisenthal more recently.
MCED occurs only in endothelial cells and not in normal or cancer cells.
MCED can be induced by certain substances that are known to be lethal to endothelial cells.
Among the MCED-inducing substances are anti-angiogenic drugs and oxidized lipids.
Other chemicals, including standard chemotherapy drugs, induce only non-MCED-mediated cell death.
MCED can be distinguished from the non-specific cell death.
MCED is an energy-dependent process that can be inhibited by non-specific cytotoxic agents and by sub-optimal culture media.
MCED involves a specific, multi-step pathway.
Immune cells appear to interact with MCED cells, suggesting that the latter present an antigenic focus.
A ligand, such as an oxidized lipid, probably interacts with a receptor and initiates an MCED cascade. This would provide a new and highly specific target for prevention and/or treatment of cardiovascular disease.
The most important cause of susceptibility to atherosclerotic coronary vascular disease probably is the presence or absence of circulating MCED factors and not cholesterol or other serum lipid levels.
It is probable that some circulating serum factors inhibit MCED while other factors promote it.
Most likely, MCED factors will be detectable and measurable in blood and other sera.
The prevalence of MCED promoting and inhibiting factors varies among different individuals.
What We Know Now; MCAD Becomes MCED
The insight that endothelial cells die through the mechanism of MCED did not spring fully-formed from Dr. Weisenthal’s intellect and imagination. For several years, Dr. Weisenthal discussed, published, and otherwise referred to his findings using the acronym MCAD, which stands for Massive Calcium Accumulation Endothelial Cell Death. The name derived from the calcium “lakes,” that form around endothelial cells undergoing this newly-discovered form of cell death. However, while MCAD was and is a defining feature of the inflammatory mechanism there is more to the story.
Through 8 years of painstaking research, marked both by encouraging successes and disappointing set-backs, Dr. Weisenthal was able to drill down further into the step-by-step process by which an endothelial cell actually dies. In doing so, he answered additional questions about what specifically causes vessels to become inflamed and obstructed.
So What is MCED?
Based on Dr. Weisenthal’s most recent research, here is his assessment of what probably happens:
Endothelial cells need substances called pro-angiogenic factors in order to stay alive. Pro-angiogenic factors work by contributing something of value to a broader pro-angiogenic pathway. In the world of cell biology, the word “pathway” is used to indicate a multi-step biochemical process. If something happens to interfere with one or more pro-angiogenic factors the entire pro-angiogenic pathway can be disrupted. When this occurs, a different pathway - one that leads to endothelial cell death by the mechanism of MCED - can be set into motion.
No matter how MCED begins, the pathway always leads to the same destination - the formation of endosomes.
An endosome is a tiny transport vesicle - think of it as a self-contained shipping department that springs spontaneously into existence, sorts-out various substances, and then either transports them into the interior of the cell or else ushers them unceremoniously back out onto the street, depending upon whether or not a specific substance is deemed useful to the cell.
When an endothelial cell is dying by the mechanism of MCED, the endosomes become highly calcified and are expelled from the cell. An endosome that is expelled from a cell changes its name and is thereafter called an exosome. As seen through a microscope, calcified exosomes cluster around dying endothelial cells like bunches of grapes.
The presence of highly-calcified exosomes and endosomes provokes a response in which the usual cast of inflammatory immune cells - monocytes, lymphocytes, neutrophils, etc. - attack what they perceive to be unwanted debris. In the course of the clean-up effort a zone of chronic inflammation arises throughout a field of dead and dying endothelial cells.
Calcification and Inflamation: A Deadly Cycle
Despite the body’s best efforts not all of the calcified endosome and exosome debris can be cleared away. And so the body does what it always does with an irritation it can’t get rid of - it tries to wall it off. It is roughly the same process that occurs when a splinter stays in the body too long or when a cyst is formed around an infection.
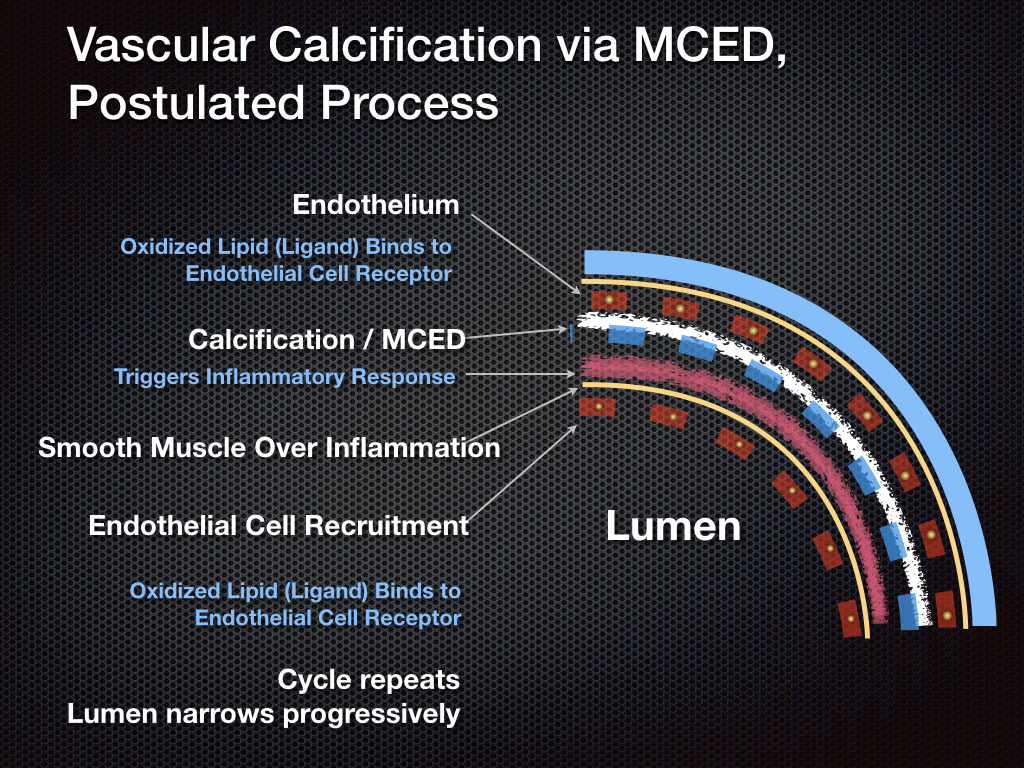
In the case of vascular MCED, the body walls-off the calcified debris and chronic inflammation by laying-down a covering of smooth muscle along the interior of the blood vessel. New endothelial cells are then recruited. These arrange themselves over the smooth muscle layer. You may recall, as stated earlier, that blood vessels are lined with endothelial cells.
Unfortunately, the new endothelial cells are now vulnerable to injury by exactly the same factors that killed the previous layer of endothelial cells. And so the whole process repeats itself. As each endothelial layer dies, becomes inflamed, and is covered-over by a new layer, the the interior of the vessel becomes narrower and narrower. This progressively restricts the flow of blood through the vessel until a blood clot is formed and stroke or heart attack results.
Dr. Weisenthal’s newest findings are important because, as more of the MCED cell-death pathway is mapped, more opportunities arise along its entire length to intervene with drugs that disrupt the pathway, block MCED, and halt or prevent vascular inflammation.
Setbacks
The MCED discovery process hasn’t always gone smoothly. There have been set-backs along the way, some of them gut-wrenching. At one point, Dr. Weisenthal lost nearly a year when MCED simply stopped working in his experiments for no apparent reason. Dr. Weisenthal finally discovered that the problem was caused by variable batches of a certain cell culture medium ingredient - one of many ingredients he uses in his medium. Diabolically, the ingredient was supposed to be identically-formulated from batch to batch and it was all purchased from the same supplier. With additional staff to conduct experiments and with money to test multiple batches of medium simultaneously he probably could have resolved the mystery in a week. Instead, short-staffed and self-funded, it took months to track down and fix the problem.
The Road Ahead - From Discovery to the Clinic
The work on MCED continues. Much has been accomplished and much work remains. But the paradigm-changing aspect - the discovery of MCED - has now been made. Identifying and isolating one or more MCED factors should be reasonably straightforward. But it requires funds and it requires bio-pharmaceutical collaborators. The purpose of this site, therefore, is to raise awareness so that this promising work can continue.